LASIK surgery is a popular procedure that many people undergo to correct their vision. It is a safe and effective way to eliminate the need for glasses or contact lenses. If you are considering Surgery Lasik, it is important to understand the procedure and what to expect during the recovery process. In this article, we will take an in-depth look at LASIK surgery, from how it works to the potential risks and complications.
Understanding LASIK Surgery
What is LASIK Surgery?
LASIK stands for Laser-Assisted In Situ Keratomileusis. It is a surgical procedure that uses a laser to reshape the cornea, improving the eye’s ability to focus. Surgery Lasik is primarily used to correct refractive errors such as nearsightedness, farsightedness, and astigmatism. By reshaping the cornea, LASIK surgery helps light to properly focus on the retina, resulting in clearer vision.
The Science Behind LASIK
The cornea is the clear, dome-shaped surface that covers the front of the eye. It plays a crucial role in focusing light onto the retina, which is responsible for transmitting visual information to the brain. When the cornea is misshapen, it can cause blurry or distorted vision.
LASIK surgery involves creating a thin flap on the cornea using a microkeratome or a femtosecond laser. This flap is then lifted, and a laser is used to remove a precise amount of corneal tissue. The surgeon carefully reshapes the cornea to correct the specific refractive error. Once the cornea is reshaped, the flap is repositioned, acting as a natural bandage.
One of the key benefits of LASIK surgery is its quick recovery time. Most patients experience improved vision almost immediately after the procedure, with minimal discomfort. The majority of patients can return to their normal activities within a day or two, making LASIK a convenient option for those with busy lifestyles.
It’s important to note that while LASIK is highly effective for many individuals, not everyone is a suitable candidate for the procedure. Factors such as age, overall eye health, and certain medical conditions can impact the success of LASIK surgery. A comprehensive eye examination and consultation with an experienced ophthalmologist are essential to determine if LASIK is the right choice for you.

Preparing for LASIK Surgery
Initial Consultation and Eye Examination
The first step in preparing for LASIK surgery is to schedule an initial consultation with a qualified ophthalmologist or eye surgeon. This consultation is a crucial step in the process as it allows the surgeon to assess your eyes thoroughly. During the examination, various tests will be conducted to determine if you are a suitable candidate for LASIK surgery. The surgeon will evaluate your prescription, corneal thickness, and overall eye health to ensure that the procedure is safe and appropriate for you.
Furthermore, the surgeon will take the time to discuss the potential risks and benefits of LASIK surgery with you. It is important to have a clear understanding of what to expect during and after the procedure. Feel free to ask any questions or express any concerns you may have during this consultation. Your comfort and confidence in the process are paramount. Read more about comfort and confidence at https://caps.umich.edu/content/helping-someone-self-esteem
Pre-Surgery Guidelines
Prior to the day of surgery, your surgeon will provide you with specific instructions to follow. These instructions are designed to help optimize the outcome of the procedure and minimize any potential risks. Some common guidelines may include:
- Avoiding the use of contact lenses for a certain period of time before surgery to ensure accurate measurements and assessments.
- Stopping the use of eye makeup, creams, or lotions on the day of surgery to reduce the risk of infection or complications during the procedure.
- Arranging for someone to drive you home after the surgery, as your vision may be temporarily impaired, and it is not safe for you to drive immediately following the procedure.
Adhering to these pre-surgery guidelines is essential to ensure that your eyes are in the best possible condition for the LASIK surgery. By following these instructions diligently, you are actively participating in your own care and setting the stage for a successful outcome.
The LASIK Procedure Step-by-Step
The Role of the Surgeon
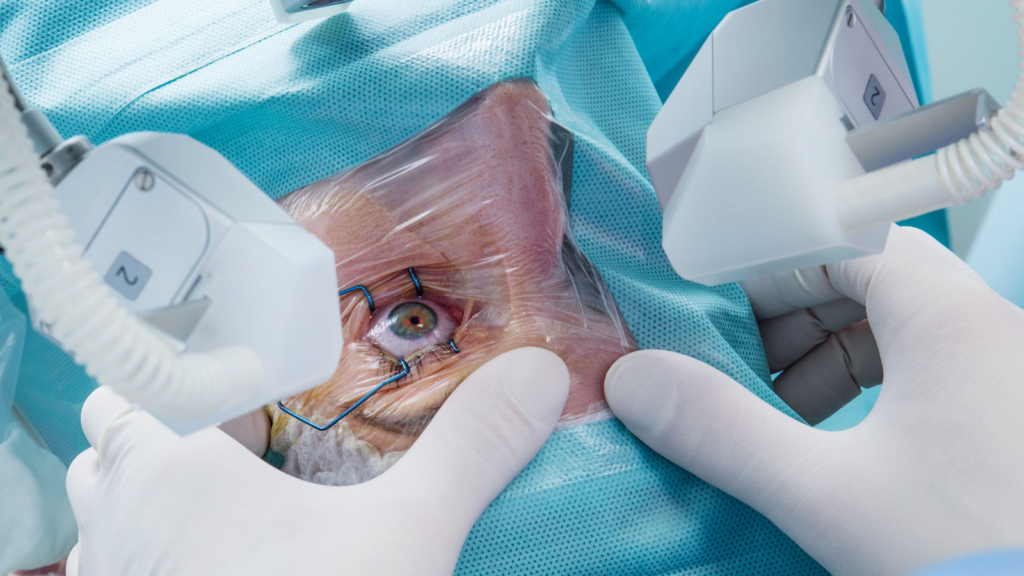
During the LASIK procedure, the surgeon plays a critical role in guiding the entire process. They will first administer numbing eye drops to ensure your comfort throughout the surgery. The surgeon will then create the corneal flap using either a microkeratome or a femtosecond laser. This part of the procedure is generally painless, although you may feel pressure on your eye.
It is important to note that the surgeon’s expertise and precision are crucial in determining the success of the LASIK procedure. Their years of training and experience allow them to perform delicate eye surgeries with accuracy and efficiency. The surgeon’s steady hand and focused concentration are essential in every step of the process, from creating the corneal flap to reshaping the cornea with the laser.
The LASIK Equipment
Advanced laser technology is used to perform LASIK surgery. The equipment used will depend on the surgeon’s preference and the technology available at the surgical center. It is essential to choose a surgeon who has experience with the latest LASIK equipment to ensure the best possible outcome.
The LASIK equipment undergoes regular maintenance and calibration to ensure optimal performance during surgeries. The precision of the laser technology is paramount in achieving accurate and predictable results for each patient. Surgeons work closely with technicians to calibrate the equipment and ensure that it meets the highest standards for safety and efficacy.
The Procedure Itself
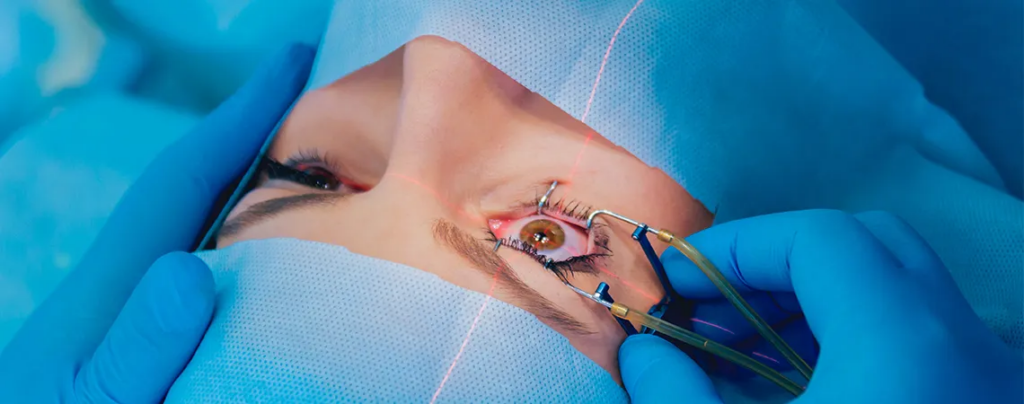
Once the corneal flap is created, the surgeon will use a laser to reshape the underlying cornea. The laser removes precise amounts of tissue, correcting the refractive error. The entire procedure typically takes less than 15 minutes per eye.
During the procedure, you will be asked to focus on a fixed point of light while the laser reshapes your cornea. You may experience some pressure or discomfort, but it should not be painful. The surgeon will guide you through the process, ensuring your comfort and safety.
It is fascinating to consider the intricate nature of the LASIK procedure, where cutting-edge technology meets the skillful hands of a trained surgeon. The collaboration between human expertise and advanced equipment results in improved vision and a better quality of life for many individuals seeking freedom from glasses or contact lenses. The LASIK procedure represents a harmonious blend of science and artistry, with the surgeon as the conductor orchestrating each precise movement to achieve optimal visual outcomes. To learn more about cutting-edge technology click here.
Post-Procedure Care and Recovery
Immediate Aftercare
After LASIK surgery, your eyes will be sensitive and may feel dry or irritated. Your surgeon will provide you with specific aftercare instructions to follow, including:
- Using prescribed eye drops to aid in the healing process
- Avoiding rubbing your eyes
- Wearing protective sunglasses outdoors
It is crucial to follow these instructions to promote proper healing and reduce the risk of infection.
Additionally, it is common to experience some sensitivity to light and glare following LASIK surgery. This sensitivity should diminish over time as your eyes heal. To help with this, you may want to consider wearing sunglasses even indoors or using computer screens with lower brightness settings.
Long-Term Care and Recovery
While most patients experience improved vision immediately after LASIK surgery, it can take several weeks or even months for your eyes to fully stabilize. During this time, you may notice fluctuations in your vision. It is essential to attend all follow-up appointments with your surgeon to monitor your progress.
Furthermore, it’s important to note that some patients may experience dry eyes as a common side effect of LASIK surgery. Your surgeon may recommend using artificial tears to help alleviate any discomfort associated with dryness. Staying hydrated by drinking plenty of water can also contribute to maintaining adequate tear production.
Long-term care involves maintaining good eye hygiene, scheduling regular eye exams, and wearing protective eyewear when necessary. By following these guidelines, you can enjoy the long-lasting benefits of LASIK surgery.

Potential Risks and Complications
Common Side Effects
As with any surgical procedure, there are potential risks and complications associated with LASIK surgery. Common side effects include temporary dryness, glare, halos, and light sensitivity. These side effects typically resolve within a few weeks or months after the procedure.
Serious Complications
While rare, serious complications can occur after LASIK surgery. These may include infections, corneal scarring, or corneal ectasia. It is crucial to discuss these potential risks with your surgeon and make an informed decision about whether LASIK surgery is right for you.
It is important to note that while LASIK surgery has a high success rate, individual outcomes can vary. Factors such as pre-existing eye conditions, age, and overall health can influence the results of the procedure. Your surgeon will conduct a thorough evaluation to determine if you are a suitable candidate for LASIK and discuss any potential factors that may affect the outcome.
Furthermore, post-operative care plays a significant role in the success of LASIK surgery. Following your surgeon’s instructions regarding eye drops, rest, and avoiding activities that may strain your eyes is crucial for a smooth recovery process. Any deviation from the recommended post-operative care guidelines could increase the risk of complications and affect the final outcome of the surgery.