Not the nicest topic I’ll grant you but nevertheless an important subject that we need to deal with. Cancer is an exceedingly stressful condition and I’m a great believer that stress/chronic stress is the biggest killer of all, regardless of what the anti-smoking nutters say or the ‘lifestyle guru’s’ profess to know! Without even trying these two factions cause people more stress than they realize – though they would never admit it. They are simply another case of the ‘do-gooders’ doing badder! Clint Eastwood has just celebrated his 88th birthday but according to the anti-tobacco & anti-alcohol mobsters, he should have had the decency to depart this world 20/30yrs ago!
We all like a drink at some time or other and the majority of us have a pint or two at the weekend or at family functions etc; ie, we drink in moderation mostly. However, lack of moderation causes its own problems, such as depression, low self-esteem, worthlessness, etc resulting, more often than not, in imbibing more and more so as to blot out the realities of life and its hardships. And, strangely enough, it works in the reverse order too!
If you remember from one of our first posts, smoking & alcohol, although contributory factors ARE NOT the main causes of oral/throat cancers. “Yes they are” I hear you yelling at me, but the truth is that the HPV (Human Papilloma Virus) is the main culprit and that virus is passed on from human to human via sexual activity mainly. The American University found that 65% of oral/throat cancers were caused by the HVP, 21% from alcohol abuse, 12% from smoking/chewing tobacco & 2% unknown/unaccountable. The strange thing is that there is no determination of ‘alcohol abuse! Does that mean 1pt of beer per day or is that 10pts per day? Is it 1 glass of wine per day or is it a bottle of wine with every evening meal?
Did you know that the ‘medical genius’ who determined how many units per day we could safely drink used no scientific formula, no tests, no mathematical equations whatsoever: he simply stated that (eg) 4 units per day for men & 2 units per day were the safe level! Some science that is – and I can tell you now that I have since seen the following sign in hospitals:- Beware-There is NO safe level of alcohol. The same route as the SHS brigade and absolute hogwash of course, but then it is their intention to use the fear factor in all matter prohibition. With smokers/smoking they got away with it but with 95% of the population enjoying a drink at some time or other ‘they’ have no chance of following the smoking route with alcohol etc.
We have been sent a very in-depth piece by a gentleman by the name of Mr Paul Bailey who knows what he is talking about, being an ex-alcoholic himself. It highlights the immense dangers of alcoholism and I do advise people to read this and take note of what can become of them.
Guide to Alcohol and Cancer. A matter-of-fact guide by Paul from “Rehab 4 Alcoholism” explaining the cancer risks associated with drinking alcohol. See more at:
I think the important thing to remember is that this view from an ex-alcoholic is simply another pointer for you all to consider. We all now know that cancer is nothing but a lottery, some will & some won’t but this is just another step in the right direction of possible avoidance.
Tonsil cancer is cancer that occurs in one of the three types of tonsils of the throat.
palatine tonsils (most common) which are located on either side of the throat
pharyngeal tonsils (also called adenoids), which sit behind the nasal cavity
lingual tonsils, which are at the back of the tongue.
always check yourself out, viz… (small torch & mirror make it easy)
The back third of your tongue
The soft area at the back of the roof of the mouth (the soft palate)
The tonsils and two ridges of tissue in front of and behind the tonsils
The back wall of your throat
Most tonsil cancers are squamous cell carcinomas, which we have previously mentioned, although it is possible for lymphoma (a type of immune system cancer) to develop in the tonsils. As with most throat cancers, it has been found that the human papilloma virus (HPV), the commonest cause being oral sex, is the single most causation. the combination of smoking and alcohol use yields an even greater risk than using either substance alone. Smoking is a common risk factor for squamous cell carcinomas of the tonsils as is alcohol:
Symptoms of tonsil cancer include a sore at the back of the throat that does not heal or one tonsil that is bigger than the other. It may or may not be painful. Tonsil cancer is known to cause bleeding, bad breath, or altered taste. Larger cancers can interfere with eating, talking, or breathing, and may make it difficult to open the mouth. Lumps on the side of the neck have also been noted.
How far your cancer has grown into local tissues
Whether it has spread to nearby lymph glands
Whether it has spread to any other part of the body – this is called staging cancer. Your doctor will be able to tell you more about which treatment is best for you once your cancer has been staged.
Radiation therapy or surgery can be effective in treating early tonsil cancer, and chemotherapy can be effective in treating more advanced tonsil cancer. Following surgery to remove cancerous tissue, reconstructive surgery can help restore structures that have been removed and rehabilitation can help you relearn how to eat, swallow or talk if needed.
Some complications of tonsil cancer can be serious. Seek immediate medical care (call 999) for serious symptoms, such as uncontrolled or heavy bleeding or respiratory or breathing problems, such as shortness of breath, difficulty breathing, labored breathing, wheezing, not breathing, or choking. You have the best chance of curing tonsil cancer if you catch it early.
Seek prompt medical care if you have bleeding in the throat, notice sores or lumps in the back of the throat, have difficulty eating, swallowing, or speaking, or have any other symptoms that concern you. please note that with tonsil cancers, if treated early enough, there is every chance that cancer will NOT spread thus causing loss of voice-box/larynx. This simple knowledge, above all else, should ensure that any worried persons should report to their doctor immediately for a full check-up.
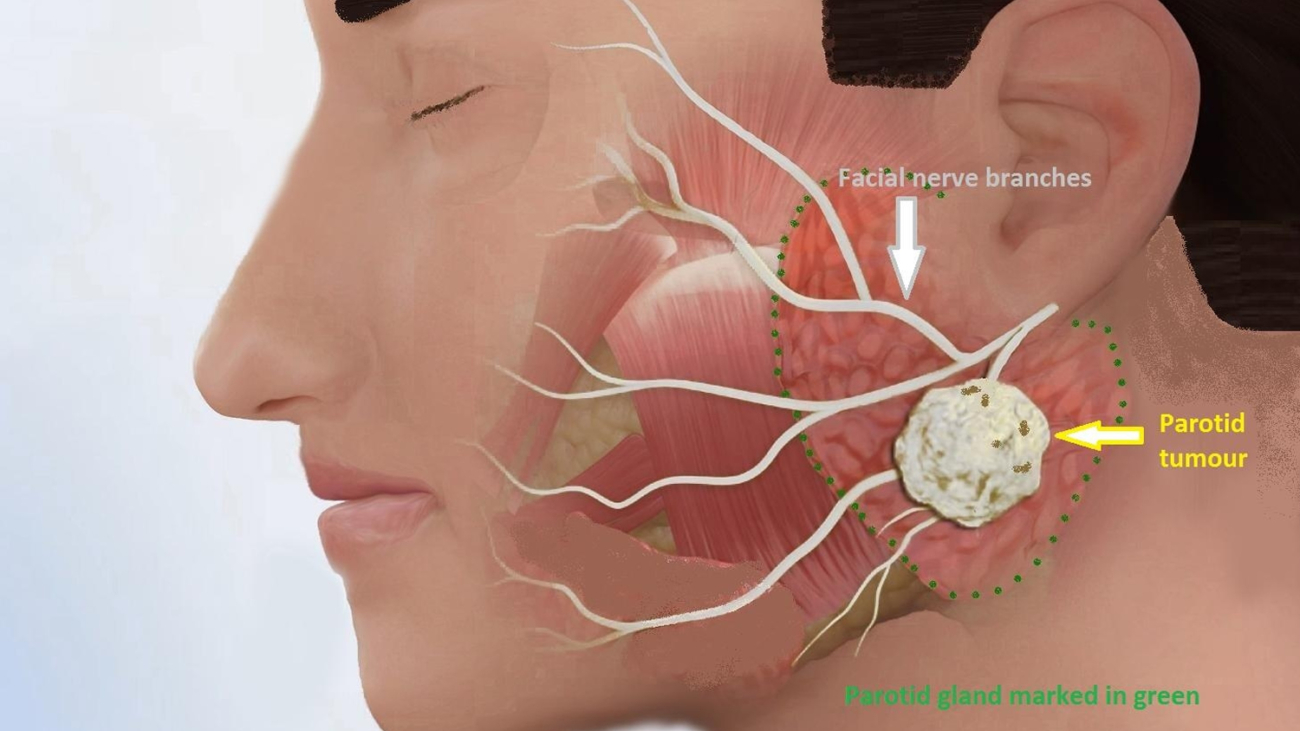
Salivary Gland cancer kills Adam Yauch (Beastie Boys) Cancer of the salivary gland is quite rare, The statistic given by NCI is 2.5 to 3 new cases out of 100,000 population, or about 1,000 new cases per year in the US – according to the National Cancer Institute. Cancer only represents 3 to 5 percent of total head and neck cancers.
Cancer begins in the salivary glands in the head, which are located in the mouth, throat, and neck. The most common place for cancer to start is in the parotid gland — near the front part of the ear.
Adam “MCA” Yauch, a member of the iconic Beastie Boys, has passed away after being diagnosed with cancer of the salivary gland, according to news reports.
Yauch, 47, was treated for cancer in 2009, and in 2011, there were false reports that he had beaten it. But he actually was never cured of the disease.
Not all salivary gland tumors are cancerous, according to the National Institutes of Health. When the tumor is benign, a doctor may choose to just remove the salivary gland. However, other treatments like radiation therapy and chemotherapy are needed if the tumor is malignant (surgery to remove the cancerous tumor is also an option), according to the Cleveland Clinic.
Salivary gland cancer is most common amongst people in their 60s and 70s, according to the National Cancer Institute. Risk factors include being exposed to radiation (like that which is used to treat other cancers in the head or neck), and exposure to substances used in asbestos mining, plumbing, and rubber manufacturing signs of salivary gland cancer include:
having a typically painless lump in the mouth or near the ear, jaw, lip, or cheek, ear fluid drainage, a numb or weak sensation in the face, problems with swallowing, and facial pain – according to the National Cancer Institute. Tests to diagnose cancer include screenings like MRI, CT or PET scans, an ultrasound exam, and endoscopy.
The Cleveland Clinic reported that a number of factors can influence how deadly salivary gland cancer will be, including how old the patient is and how healthy he or she is; what kinds of cancer cells the tumor is comprised of; which salivary gland the cancer is in; and the size of the cancer tumor.
*****
Salivary Cancer-general information
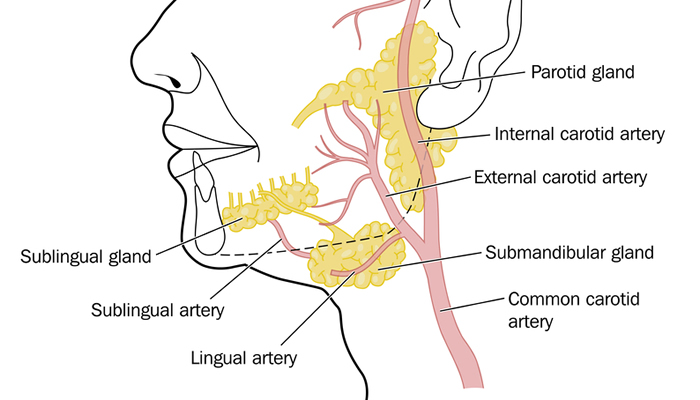
The salivary glands make saliva (spit). This keeps your mouth moist and helps food slide down the gullet into the stomach. The largest salivary glands are the:
sublingual glands, which are found underneath the tongue
parotid glands, which are found at the sides of the mouth just in front of the ears
submandibular glands, which are found under the jawbone.
There are also many more tiny glands in the lining of the mouth and throat. These don’t have individual names but are known as the minor salivary glands and cancers affecting the salivary glands are rare, with approximately 550 new cases in the UK each year. They can occur at any age but are more common in people over 50. There are different types of salivary gland cancer, depending on the type of cell that has become cancerous.
Like many other forms of cancer, the exact causes of salivary gland cancer are unknown. Non-cancerous tumors of the salivary glands are a lot more common than cancerous tumors apparently!
Tumours affecting the salivary glands are not infectious and cannot be passed on to other people. They are not caused by an inherited faulty gene, so the relatives of someone with salivary gland cancer won’t be queuing up for a bout of salivary cancer!
Things to look out for are swelling on the side of the face, just in front of the ears, or under the jawbone and some people suffer some numbness and drooping of one side of the face (facial palsy)-a bit like having a stroke.
These symptoms may occur with different conditions; ie, other than cancer, and most people with these symptoms won’t have a salivary gland cancer-very few do. However, like most cancers, salivary gland cancers are best treated when diagnosed at an early stage. You should tell your GP about these symptoms if they do not improve over a few days.
I have read through what KB has to say and I think it may well be of value to many of you out there, for, at the end of the day, cancer is cancer and anything that helps has to be a bonus ball. I state here and now that we may not agree with all that is written & there will be bracketed opinions along the way but each person must make up their own mind as we go along! I hope they’ll ease the minds of anyone going through a difficult time due to a cancer diagnosis.
Nine ways to reduce your cancer risk:
1… Don’t smoke – or use any form of tobacco. If you’ve never smoked or have already quit, congratulations – you don’t have to do a thing. If you do smoke or use tobacco products, you can cut your cancer risk by stopping right now. Quitting isn’t so easy, but the benefits are almost instantaneous: Medical experts have found that a person’s health can improve within minutes of the last puff (or snuff) – and the health advantages can last a lifetime. Here’s a simple step-by-step plan to get you started.
(Having stated the above, one has to remember that smoking/snuffing/vaping is a freedom of choice & some people are simply born to smoke, and some do not. It is also worth remembering that the six (6) oldest people ever to live all smoked for at least 70 years! Another couple of interesting facts are that 80% of lung cancer cases occur in NON-smokers & 49% of lung transplants come FROM smokers/ex-smokers. Smoking does NOT actually cause lung cancers but it is a ‘risk factor). Bizarrely, back in the mid 60’s the then Surgeon General USA (Dr Richard Carmona) declared that even standing next to a smoker (smoking) could give you cancer/cause you to have cancer – but never a mention of the highly toxic & dangerous road traffic fumes! (food for thought there).
2… Make your home (and car) smoke-free. Okay, so you don’t use tobacco, but is the rest of your life up in smoke? All the cancer-causing ingredients in cigarettes, cigars, and pipes are also found in secondhand smoke. Even the remnants of tobacco smoke on surfaces, known as thirdhand smoke, can be a health hazard. If you live with a smoker, ask him or her to quit – or to smoke outside, away from your home or car. Adults, kids, and even pets are all at risk from the danger of secondhand and thirdhand smoke.
(Firstly, it is impossible to make your home or car smoke-free. Secondly, SHS has now been officially declared harmless by the WHO, which is a total backtrack on all the lies spouted a decade ago so as to gain smoking bans worldwide! True scientific research has caught up with the WHO and they now have little option but to comply with the truth which is simply that as the world became more & more industrial so did cancers become more prevalent.
As for harmless ‘third-hand smoke’, [only a theory by the way] so-called by Dr Winnickoff, who put the telephone down on me some years ago, it is basically a scaremongering tactic that quickly gained worldwide recognition as a household danger [courtesy of the ever greedy media, etc] -but then so are dust particles, cooking odours, air pollution generally – and a whole host of other things that you wouldn’t even think about – that’s why we now have ‘antiseptic wipes’ and ‘Dettol sprays’ these days. By the very nature of the beast, it is impossible to avoid airborne toxins when driving the car or simply traveling in a car! Either fumes from the car in front, behind, next to you, or you own car will get to you for the simple reason that they are forced out of the car via the exhaust system. However, rigorous testing has proven unequivocally that a window or two, opened only 1/2″, will greatly help to dissipate all such unseeable fumes.)
Asbestos – What You Need to Know:
This section deals with the dangers of asbestos, a much-used material back in the late 40’s & 50’s as it was cheap, very usable, and easy to get hold of! Now, most of this is written for our American friends but I will point out that over here in Britain the easiest way to dispel fears of asbestos if refurbishing a property was to leave it in situ if possible, especially as a dividing wall [which it often was], and simply PVA (which seals the outer surface) & plasterboard straight over it, then a double coat of plaster! Simple, cheap, and very effective.
You see good people, where folks go wrong is they adhere to all the scaremongering and think they need to call in the very expensive ‘professional asbestos removers‘ [who look like spacemen in all their protective gear] when in actual fact they don’t! I know of an elderly gentleman who had an old style ‘asbestos sheet garage‘ that needed clearing out: the council informed him that there would be an £800-£900 charge.
A few lusty blows in the right places soon razed said garage to the ground, leaving for 30 minutes to let those nasty little spores dissipate/settle and the offending asbestos was quietly bagged up and taken to the local tip – total cost…..£3 in petrol!
Wearing a protective mask is always a great idea when dealing with any asbestos as the airborne spores do not do anyone any favors but generally, if asbestos is treated with respect there is very little danger of it causing any form of cancer. You may well laugh but it is not a bad idea to gently ‘hoover up over the old concrete base so as to be clear of any random spores. As always, it is up to the individual as to what they decide to do with their asbestos-if they even have any.
ASBESTOS 11:
This is a detailed composition of how you should go about removing any asbestos in your home – American style – with costs ranging from $1,000 & $2,500 and involving people dressed as spacemen for the duration of their removals. As per normal you are treated as if you are dealing with ‘sarin gas‘; ie, well OTT and most of you will find it far easier to follow my route (which is not illegal) as detailed above.
Creative play – Helping children cope with cancer:
This department is way beyond my humble knowledge so we’ll rely on all the good work done by ‘KB’ and simply pass the information onto our good selves.
This is a very tricky area to go into and best left to the professionals but I do know of a couple of ‘characters’ who chose their own path and drank until the day they passed away. Now whether the drink subdued the physical or mental pain I know not, but they simply did what suited them so who can really argue with that? One thing that is for sure is that no one single person can state exactly how the next person should be feeling when the news hits them nor how they will react. So, read all of these ‘mini-chapters’ carefully prepared by ‘KB’, and perhaps something will be of help to you or a loved one who has embarked on this rocky path. Good luck to you all.
I also know of cannabis smokers who swear by the plant for easing the aches & pains of cancer and I could never ‘knock them’ for using the stuff. The law, in Britain, is an ass as far as cannabis use is concerned but, as is our way, if the Judiciary see a simple way of making money through criminal proceedings (fines, etc) then they will not change a stupid law that would benefit so many people in so many ways – especially those suffering from the many forms of terminal cancer! Though having never used cannabis myself I would not hesitate to purchase some for a loved one if it eased their pain.
Interestingly the latest studies/research/findings have all concluded that obesity is a major cause of cancer. Not ‘A’ cancer but ALL cancers if you please. Now we know that all the lies, all the manipulations, all the fabrications prior to the implementation of the smoking bans are coming apart at the seams because, to the horror of the medical profession, cancer cases are still rising on a daily basis (now at 900 new cases per day – Macmillan).
We already have the proof that the vast majority of head/neck/throat cancers are caused by the Human Papilloma Virus and a recent study has simplified matters even more by declaring that it is literally 50/50 as to whether you are lumbered with some form of cancer or not! (For those that might be interested: the HPV study found that 65% were due to oral sex, 21% due to alcohol consumption & 14% due to smoking). Now that obesity has been thrown into the mix it will be interesting to see how the figures are massaged to suit – though to be fair, obesity does cover ALL types of cancer!
So that proves that all the medical hype behind the greatest destruction of any social environment was simply at the behest of ‘Big Pharma’ and those that detest tobacco usage in any form.
“Cancer deaths are soaring in parts of the UK with the highest obesity levels, new figures have revealed. In pockets of the country where vast swathes of the population are overweight, rates of the disease are rocketing.” –Campaigners warned today if drastic action is not taken to stem the rising tide of obese and overweight people, cancer will continue to claim more and more lives.
There you have it, folks, you already know what the next tobacco is going to be (after sugar & alcohol of course!)
After the war we had lean times where the man went to work, woman tended the home & some of the gardening-man produced crops at evening time & weekends – usually before disappearing off down to the pub! What this did was create a homegrown vegetable economy, which of course has now long since passed as we mostly buy vegetables by the bag or tin, these days.
The other important factor we need to take on board is the fact that since the first Wimpy Bar opened in the early 60s, there has been an explosion of cafes, takeaway joints & snack bars. Anyone can now eat virtually any type of food at any time of the day or night… ‘eating on the hoof‘ has fast become the norm as our daily life becomes ever more hectic.
High unemployment/retirement areas seem to be the fattest!
Again, after the war, industrialization boomed. There were jobs aplenty as businesses thrived in post-war Britain but the silent killer was also on the increase, whilst smoking rates (72%-75% in the late ’50s) started to diminish (25% – 2005), as more people decided for themselves not to smoke. With the rapid increase in industrialization came the inevitable cancerous death toll – yet hardly anyone put the two together!
Now, of course, we have the anti-smoking lobby sitting there simply waiting for any excuse to blame the poor old tobacco plant for all the world’s ills. It is so simple for them to do so and also keeps their funding in place from various sources. Should their funding ever be withdrawn I dread to think what the likes of ASH, FRESH, etc will do for finance because public donations will amount to very little indeed.
Note the lowest obesity figures in busy, busy London!
It is interesting to note that they (the medical profession/governments/lobby groups) are fast running out of things to hide behind as major causes of cancers (air pollution is the latest!) for back in the 1980’s one woman dedicated her life to ascertaining what mostly causes cancers.
Dr. Kitty Little blew the lid on the causation factor by announcing that diesel fumes & industrialization were, without doubt, the major causes of cancers developing – she was hushed up, silenced, ignored, etc as it didn’t suit the then-new anti-smoking agenda, lead by that eminent tobacco hater Sir George Edward Godber at that time. Strangely enough, the World Health Organisation (a complete & utterly disgusting dictatorship) finally came out of the closet and agreed with her findings-but not until the worldwide destruction of people’s choices & social structures had taken place! Strange that the WHO will happily allow 4,000 people per day to die in places like Africa through disease, and lack of food/water, yet will waste $bns on tobacco cessation!
We have to ask the question here: who allowed all these ‘takeaway’ businesses to flourish in this country? The Friday night treat, when I was a kid, was fish n chips from the corner chippy-and oh boy, it was a treat. But now….. well, you can go out all night, drink, be merry and grab a Chinese, Indian, Turkish, Thai, or whatever other culinary delight tickles your tastebuds and stagger home ‘filling your face’. (hence the abundance of ‘fast food’ litter each day to be cleaned up!
So you see folks, we have bred a culture whereby we have created the perfect storm for deadly diseases like cancer. We eat, we drink, we smoke, we ‘slob out and more of us die from cancer but the flip side is that we are only here once so we enjoy whatever time we have on this planet. Cancers will always abound and they will always be a statistical victor too as they will always claim lives-age is no barrier to cancer I can assure you!
I am also fairly certain that we will end up going ‘full circle as there is much ‘hoo-haa’ about the dangers of crop-spraying etc so the time is now approaching where homegrown vegetables will once again be a booming but safe industry. Allotments are becoming more fashionable again as people try to cut down on the general cost of living – and with the use of ‘freezers’, any amount of fresh vegetables can be semi-cooked & frozen for use at a later date.
What we do have to remember is that cancerous cells are in every single one of us, it just takes something to trigger off the mutations. Once those mutations have been triggered it is then up to the medical world to act quickly and either remove the offending cells (ie, invasive surgery) or ‘kill’ them off (chemo/radiation). It is the speed with which these cells are dealt with that determines the patient’s longevity and that is why we at “20-20 Voice” Cancer are simply ‘hell-bent’ on providing the up-to-the-minute technology to our local hospitals – and that is where you can help us!
I have set up a personal page on the MyDonate website where the aim is to reach £1,000,000.00, for that is what we need to be able to buy the equipment required to provide the all-important diagnostics for head, neck & throat cancers. All donations go directly to “20-20 Voice” Cancer and every penny counts so we would be very appreciative of your donation. Thank you all.
This may not be the best subject for many to read about but it remains a sad fact that suicide rates amongst laryngectomees are 3x higher than any ‘normal’ suicide rates!
Patients with head and neck cancer have more than 3 times the incidence of suicide compared with the general population, with rates highest among patients with cancers of the larynx and hypopharynx, according to a study published by JAMA Otolaryngology-Head & Neck Surgery.
Dr Itzhak Brook has written the following and his words should be heeded!
High Suicide Rate for Patients with Head and Neck Cancer
Patients with head and neck cancer have more than 3 times the incidence of suicide compared with the general population, with rates highest among patients with cancers of the larynx and hypopharynx, according to a study published by JAMAOtolaryngology-Head & Neck Surgery.
Dr. Chan Woo Park R, M.D., of Rutgers New Jersey Medical School, Newark, and colleagues examined the incidence rate, trends, and risk factors of suicide in patients with cancer of the head and neck between 1973 and 2011. Compared with the suicide rate of the general population, the researchers found that patients with head and neck cancer have more than 3 times the incidence of suicide. Suicide rates were higher in those treated with radiation alone compared with those treated with surgery alone.
There was a nearly 12-fold higher incidence of suicide in patients with hypopharyngeal cancer and a 5-fold higher incidence in those with laryngeal cancer. The authors suggested that this may be linked to these anatomic sites’ intimate relationship with the ability to speak and/or swallow and that loss of these functions can dramatically lower patients’ quality of life. It is possible that the increased rates of tracheostomy dependence and dysphagia [difficulty swallowing] and/or gastrostomy tube dependence in these patients are exacerbating factors in the increased rate of suicide observed.
The authors recommended that additional research and effort should also be devoted to the psychological toll that cancer, treatments, and resulting morbidity have on patients.
Have you ever contemplated life without words? Try being ‘speechless’ for five minutes or just an hour! Jot down all the things you would have said in those 60 minutes you’ll be amazed at the copious amounts of writing! You will also be amazed at how many people are unable to decipher your ‘mouthing’ of simple words-ask for a cup of tea as you normally word have but without sound, try telling someone you are in pain, discuss what you want for dinner, try calling for help! I think you get the point by now folks! It will shock you!
Now imagine going into hospital for a 10-minute investigative ‘mini-op’ to check something inside your throat, but waking up 2 1/2 hours later with ‘scaffolding’ sticking out of the front of your neck. Imagine the horror of realizing that suddenly, all of that which you took for granted has gone and has been replaced by a piece of plastic pipe, and worse still, you now rely on this piece of pipe for your breathing! It’s a good job that you are laying down for the shock would ‘flat-pack’ you as the ‘full horror of the thing’ sinks in.
You’ve actually undergone a tracheotomy (and/with the possibility of a full 9-10.5hr laryngectomy to come) because when the surgeons opened up your neck they found your windpipe & food pipe pushed 2 inches back into your neck, thanks to a virulent tumor (quite possibly a rather gruesomely named ‘squamous cell carcinoma’), so they had no option, otherwise, you would have died.
That which had caused you discomfort, pain, aggravation, restricted your eating, made even swallowing liquids a chore, cut your breath whilst sleeping, caused much shortness of breath doing even the simplest of tasks was a massive tumor in your throat (imagine forcing a golf ball in there!). It had almost annihilated your larynx and was rapidly setting about annihilating YOU via strangulation – who needs the hang man’s noose! The first operation kept you alive but the second (full laryngectomy) was to kill the tumor-‘lock, stock, and two smokin’ lymph nodes!
Welcome to the world of the laryngectomee!
After 12 ½ hours of life-saving major surgery, being voiceless doesn’t seem quite so bad after all! You still have your life and if you are lucky enough to have the love of a good woman as well, then the upward learning curve begins immediately!
Many will immediately think, “ oh well, if you smoke, what do you expect!” but, would they be right in that assumption?
***All we need are 50,000 x £1 coins!***
A virus spread during oral sex is now the main cause of throat cancer in people under 50, scientists have warned. Cancers of the mouth and oropharynx – the top of the throat – used to be mainly diagnosed in older men who drink or smoke. But increasingly, it is being seen in younger men.
Prof Maura Gillison of Ohio State University in Columbus said that sexually transmitted HPV was a bigger cause of some oral cancers than tobacco.
Your doctor will refer you to your local hospital, the ENT department where they have all the equipment to investigate your troublesome neck & throat. This involves a bit of gentle prodding and poking around but if your ENT specialist can’t ascertain the reason for your referral he/she may well employ a very long, thin camera (nasendoscopy) that is inserted into your nostril and gently positioned in your throat so that a clearer picture can be acquired. This may result in your needing biopsies being taken, which involves a quick theatre ‘knock out’ and small sections of the affected area being taken for analysis.
***All we need are 25,000 x £2 coins!***
Though a marvelous invention the nasoendoscope does not give a very good picture, which of course makes the decision of the cancer specialist a damn sight more difficult when in actual fact ‘all-speed’ is necessary
However, technology advances at a tremendous rate and “Olympus” have designed a fantastic new camera known as the “Rhino-Laryngol Videoscope”, which works on the same principle as the abovementioned but with a massive difference.
Micro technology has seen a special chip inserted into the tiny camera which then transports a brilliantly clear, color picture onto as big as a 30” TV screen. Previous images were 1/10th of the size so you can imagine just how quickly and how much simpler a diagnosis could now be. Imagine a tea candle on soup plate!
*** All we need are 100,000 50p pieces! ***
To the patient it means that after chemo/radiotherapy has finished and the throat has healed somewhat, instead of going ‘through the tunnel’ (in which it is impossible to remain absolutely motionless), your consultant can look for himself with the new “Rhino-Laryngol Videoscope” and see immediately if the area is now tumor free; ie no cancer!
This has massive benefits to not only the patient but to the hospital as well. The patient gets to know the outcome of the chemo/radiotherapy a lot quicker for although the ‘scanner’ can say there are no tumors/growths left it is not a sure-fire solution-especially if the tumor is lurking in the trachea or larynx. Decisions for Head & Neck cancer patients are difficult enough at the best of times, so any time delays exacerbate the stress of those decisions.
It is always better to know than to be left guessing! It means that patients can move on a surgical procedure much quicker which not only relieves the stress factor but curtails the growth of the offending tumor. I would surmise that it will also tell the Head & Neck cancer experts whether bothering with radio/chemotherapy is actually worthwhile, therefore giving an option of going straight to surgery.
Secondly, it can save the valuable time of your consultant and the cancer specialists, for faster diagnosis means less time spent per patient thus more economical for the hospital concerned. This is not to say that your consultant, or any of the team, will deprive you of necessary time concerning any part of your treatment, merely a fact of life that even though smoking has been on a reductive trend since the 1960’s cancer prevalence has steadily increased in the same period: more patients need to be seen in the same amount of time! For instance, the smoking ban was introduced on July 1st, 2007 yet in that year alone we saw a 4% increase in cancer cases (M) & 3.75% (F) (Office of National Statistics). Therefore it is imperative that specialists are able to diagnose correctly and speedily for all concerned.
***All we need are 250,000 x 20p pieces!***
This new technological breakthrough comes at a price, however, but there is never gain without pain! At £50,000 a time the “Rhino-Laryngol Videoscope” is not a cheap investment but it IS the epitome of ‘on spot diagnosis. The mere fact that a patient’s larynx etc can be seen so clearly on such a large screen can only be a bonus as any ‘untoward cells’ will be easily spotted by the experts-thus treatments will be quicker. Imagine looking at a picture on a tea candle and then on a soup plate-that is the difference this superb piece of kit makes.
It is obvious that with us being in the grip of ‘government austerity’, expensive items like this are not exactly on the ‘urgently required’ spending list, but they should be for they can go where only investigative surgery went before. Investigative surgery is expensive, time-consuming, and can be extremely distressing for the patient (and also includes post-operative care), this wonderful innovation can save all of that.
*** All we need are 10,000 x £5 notes! ***
It is not only the ‘spotting’ of cancerous tissue that this machine will perform as skilled speech therapists will be able to assess throat muscles in dysphagic clients (clients with swallowing problems to me & you!) It provides the clinician with accurate information and the client with an informed choice-mega important, as I have found out since November 2010!
Voicetherapy can also be trialed, ie, exercises to improve laryngeal movement and therefore improve voice quality. This therapy will also have an impact on improving speech quality if it has been affected.
This assessment is particularly useful to perform with clients who have had head and neck cancer, ie, those that have undergone oral and/or oral pharyngeal surgery as they have reduced sensation and can tolerate the assessment better than those that haven’t had surgery. This advancement in technology is incredible as it opens up a completely new visual world concerning Head & Neck cancers.
It is a ‘must-have’, simple as that.
Do you know how I know all this, not being of the medical profession? Because had this technological advance been in use in April 2010, I would not have suffered as I did (no fault of the specialist team I hasten to add) until November of that year when firstly I underwent a life-saving tracheotomy and then, two weeks later, a full scale 10 1/2 hr laryngectomy! This piece of equipment would have shown any consultant that the chemo/radiotherapy had not killed off the tumor which was slowly strangling me. It was almost 7 months before my consultant opened me up to find that said tumor had forced my windpipe & food pipe 2” (two inches) into the back of my neck! No wonder I was struggling to eat, breathe and even sleep!
No wonder driving the car was becoming a ‘no-no’ as it made me doze off!
No wonder a brisk walk to the post box seemed like a marathon all of a sudden!
*** All we need are 5,000 x £10 notes! ***
This new “Rhino-Laryngol Videoscope” would not only have picked up any abnormalities in my laryngeal area, but it would also have magnified them onto a 30” screen for all to see. I sometimes wonder how much all those hospital visits and check-ups actually cost the NHS during those horrendous 7 months.
*** All we need is your help! ***
Technology means that the sooner this piece of equipment can be paid for the sooner patients can receive the best treatment possible from their dedicated Head & Neck cancer specialists.
TheLeicester Royal Infirmary (Kinmonth Ward) leads the way in plastic reconstructions for cancer patients and for all head, neck & throat cancers therefore patients from all surrounding counties will benefit from the speed & advanced definition of this new “Rhino-Laryngol Videoscope” will bring to sufferers of this terrible disease.
Now you have read all the above, please take a moment to watch this marvelous video clip of Jeremy Vine’s throat & voicebox! This is what a laryngoscope can show you!
Please donate whatever you can to this worthy cause for the sooner this piece of equipment is in situ, the sooner ENT patients will get a quicker & clearer diagnosis which will save them much worry and the overstretched hospital staff valuable time, not to mention the NHS considerable expenditure-
it’s a WIN/WIN situation all ways round!
*****
The Operation & Post Op
This next part is not for the faint-hearted, but as with all illnesses, there are gorey parts. We have included this video to show you exactly what cancer does to a larynx and when you see it after it has been removed you will see how vital it is that we strive to buy this essential RhinoLaryngoscope for future head & neck cancer sufferers.
Scottsdale, Ariz., February 20, 2014—A retrospective analysis of oropharyngeal patients with recurrence of disease after primary therapy in the Radiation Therapy Oncology Group (RTOG) studies 0129 or 0522 found that HPV-positive patients had a higher overall survival (OS) rate than HPV-negative patients (at two years post-treatment, 54.6 percent vs. 27.6 percent, respectively), according to research presented today at the 2014 Multidisciplinary Head and Neck Cancer Symposium.
The analysis included 181 patients with stage III-IV oropharyngeal squamous cell carcinoma (OPSCC) with known HPV status (HPV-positive = 105; HPV-negative = 76), and cancer progression that was local, regional, and/or distant after completion of primary cisplatin-based chemotherapy and radiation therapy (standard vs. accelerated fractionation (AFX)) in RTOG 0129 or cisplatin-AFX with or without cetuximab in RTOG 0522. Tumor status was determined by a surrogate, p16 immunohistochemistry.
The median time to progression was virtually the same for HPV-positive and HPV-negative patients (8.2 months vs. 7.3 months, respectively). Increased risk of death in univariate analysis was associated with high tumor stage at diagnosis (T4 vs. T2-T3), fewer on-protocol cisplatin cycles (≤1 vs. 2-3), and distant vs. local/regional recurrent (for all, hazard ratios (HRs) >2.0 and p<0.05). The risk of death after disease progression increased by 1 percent per cigarette pack-year at diagnosis. Rates were estimated by Kaplan-Meier method and compared by log-rank. HRs were estimated by Cox proportional hazards models and stratified by treatment protocol.
In addition, HPV-positive and HPV-negative patients who underwent surgery after cancer recurrence also experienced improved OS compared to those who did not undergo surgery. (The effect may have been more pronounced among HPV-positive than HPV-negative patients.) Recurrence is most common in the lungs for both groups of patients.
“Our findings demonstrate that HPV-positive OPSCC patients have significantly improved survival after progression of disease when compared with HPV-negative patients. Median survival after disease progression was strikingly longer for HPV-positive than HPV-negative patients,” said lead author Carole Fakhry, MD, MPH, assistant professor in the Department of Otolaryngology-Head and Neck Surgery at Johns Hopkins Medicine in Baltimore. “These findings provide us with valuable knowledge to better counsel and treat patients.”
Now any pre-op patient with half a brain would want to know what is on the other side; ie, what the situation is for themselves AFTER the life-saving operation – wouldn’t you? Many hospitals are very much on the side of post-op larys having the opportunity to talk through the situation to pre-op, extremely nervous patients, after all, losing one’s greatest form of communication is a terrifying prospect.
On the other hand, we have many hospitals who (somehow) think that post-ops talking to pre-ops is a bad move; ie, the opportunity to discuss with a post-op is simply is not entertained – WHY? What does a freshman out of medical school know about being a laryngectomee?
What does a fully qualified surgeon, even with 100 operation notches on his gunbelt, know about being a laryngectomee? The answer my friends is not ‘blowing in the wind‘ as the answer is simply NOTHING AT ALL. You cannot possibly have any idea what post-surgery feels like unless you have experienced it for yourself – and I would not advocate you try it just for the hell of it!
Hospitals that frown upon pre-ops being allowed the pearls of wisdom from post-ops are simply NOT doing their emotional bit for their patients; they are simply regressive, Luddites living in the dark ages thinking that a cheery smile and dismissive wave of the hand will suffice – I pity them and the numbskulls that sit behind desks in judgement!
Hospitals that fully support post-ops talking (counselling) pre-ops areprogressive for they can easily see the benefits of the new, fearful patient having things explained to them by those that have already ‘been through the mill‘, those that know the pain, the heartache, the silence of self & the frustration of becoming a laryngectomee are the hospitals that you want to be with for they are the ones that WANT to help you to the best of THEIR ability whereas the regressive (above described) know the surgical side inside out but care not much about the emotional side of things for it is totally heartless to deny a pre-op the all calming knowledge that a post-op can impart.
The benefits of the pre-op knowledge (from a post-op) are simply endless with the main facet being that putting the pre-op’s mind at ease is the greatest benefit to that pre-op. To have someone take away the fear of being a laryngectomee is literally priceless for fear of the unknown has always been the dread of mankind. Think about these simple facts if you will please (you are the very nervous pre-op):
a… You are communicating with a laryngectomee in person
b… They have a robotic (Dalek) voice but still talk
c… They are sitting in front of you, so they survived
d… They travel to the hospital so they are not crippled or bedridden
e… They may be back at work which has to be amazing
f… They go out in public to a pub/restaurant
g… They answer your questions honestly
h… They simply put your mind at rest
OK, folks, there are a few positives – and there can be NO negatives to having the prior knowledge (unless you simply don’t want any prior knowledge of course)! We all know that ‘coming round’ after a major operation is a long & slow process and the first few days are not going to be that pleasant but the body is an amazing creation for it always seeks to repair itself.
Even better than that is the fact that your nurses know exactly what you have been through and check on you every 15 minutes through the first 24hrs (the reason we are buying this monitor for our local hospital Lary ward) & then every hour once the body has settled down. You can take tiny sips of water to freshen your teeth/gums up a bit and in the back of your mind, you know that many before you have survived to tell the tale. It’s all upwards & onwards from thereon my friends!
To be denied the opportunity of having the whole shebang explained to you by a post-op lady is simply cruel and no one facing this operation should be denied this opportunity. If you want to know then the knowledge is there but if you don’t and wish to remain in ignorance then at least that is YOUR freedom of choice!
Mouth cancers are the most common cancers which affect the head and neck area. They can begin in any of the parts of the mouth mentioned above.
Around 1,400 people are diagnosed with cancer of the tongue each year in the UK and 1,500 are diagnosed with cancers affecting other parts of the mouth. Cancer of the lip is uncommon, with fewer than 300 people diagnosed with it every year.
Mouth cancer is more common in people over 50 and it usually affects more men than women. Most mouth cancers develop from cells that line the mouth or cover the tongue and are called squamous cell cancers.
The main causes of mouth cancers are life’s general pleasures of smoking and drinking heavily and the risk is greater if you do both, but always remember that 80% of all lung cancers occur in NONsmokers! Other causes include chewing tobacco or chewing betel or paan, which is a cultural tradition in some Asian communities.
There are other things that may increase the risk of getting mouth cancer, such as eating a poor diet and not cleaning your teeth, or seeing a dentist regularly enough. Having a weakened immune system or a virus called the human papilloma virus (HPV) (63%) are also possible risk factors. Being exposed to sunlight over a long period of time is a risk factor for cancer of the lip.
Mouth cancer, like other cancers, isn’t infectious and can’t be passed on to other people.
The two most common symptoms of mouth cancer are:
a mouth ulcer that refuses to heal
discomfort or pain in the mouth that doesn’t go away.
Not everyone has pain or an ulcer. Other symptoms include:
a white (leukoplakia) or red (erythroplakia) patch in the mouth or throat that doesn’t go away
a lump or thickening on the lip, or in the mouth or throat
difficulty or pain with chewing, swallowing, or speaking
bleeding or numbness in the mouth
loose teeth for no obvious reason
a lump in the neck
a lot of weight loss over a short time
bad breath (halitosis).
These symptoms are common in conditions other than cancer. However, if you have any of these symptoms it is important to let your doctor or dentist know straight away. Mouth cancer can be treated more successfully when it’s diagnosed early.
There are two parts to your tongue, the oral tongue and the base of the tongue. Cancer can develop in either. The oral tongue is the part you see when you poke your tongue out at someone, the front two-thirds of your tongue. Cancers that develop in this part of the tongue come under a group of cancers called oral cancer.
The base of the tongue is the back third of the tongue (nb: Michael Douglas). This part is very near your throat (pharynx). Cancers that develop in this part are called oropharyngeal cancers (pronounced oar-o-farin-gee-al).
Types of tongue cancer
The most common type of tongue cancer is squamous cell carcinoma (SCCA). Squamous cells are the flat, skin-like cells that cover the lining of the mouth, nose, larynx, thyroid, and throat. Squamous cell carcinoma is the name given to cancer that starts in these cells.
Symptoms of tongue cancer
The symptoms of tongue cancer may include
Red/white patch/es on the tongue, that will not go away
A never-ending sore throat that refuses to settle down
A consistent sore spot on the tongue
Pain or slight spasms when swallowing
Continuous numbness in the mouth
Unexplained bleeding from a noninjured tongue
Sometimes even a pain in the ear, though this is very rare indeed
Do bear in mind that these symptoms may be due to a less serious medical condition. But it is important to check symptoms with your GP just to make sure. However, there are many GPs who simply don’t have the knowledge so if the symptoms persist – you persist and get a second opinion! (Michael Douglas was found to have ‘back of tongue cancer’ by his 4th Dr – a specialist)
Risks and causes of tongue cancer
We don’t know the exact causes of most head and neck cancers, but several risk factors have been identified, the largest factor being HPV @ 63%. The rapid increase in these types of cancer has been put down to a relaxing society from the 60’s onwards-‘free love’, ‘flower power’ etc, and the main cause in the older generation has been oral sex. Needless to say, smoking/chewing tobacco (cigarettes, cigars, and pipes) has been named & shamed though it only accounts for 12% of cases whereas drinking a lot of alcohol comes in at 23% (unknowns = 2%) There is information about the risks and causes of mouth cancer in the mouth cancer section.